

By: Tyler Q. Kirk, MD
VOLUME 1 | ISSUE 1
For over a decade, Kirk Eye Center has viewed selective laser trabeculoplasty (SLT) as a first-line option for newly diagnosed glaucoma management. We immediately recognized its benefits over topical drop therapy; continuous action, no dependence on compliance, no serious long term side effects, repeatability, and efficacy. In 2019, the laser in glaucoma and ocular hypertension (LiGHT) trial, and then multiple subsequent follow up publications through 6 years post treatment initiation have confirmed our initial beliefs that interventional glaucoma better serves glaucoma patients over topical drop therapy. The LiGHT trial found better intraocular pressure control, less visual field loss, and less need for more serious filtration surgery in patients who adopt SLT early in their treatment course. If diagnosed with open angle glaucoma, the surgeons at Kirk Eye Center would all prefer SLT prior to initiating eye drop therapy on our own eyes, and that is why we encourage first line SLT therapy to our patients.

Why Interventional Glaucoma?
The problem with glaucoma drops, is your patient is unlikely to take them, and if they do take them, they are unlikely to get them in with regularity, and if they do get them in, they are likely to have unwanted side effects. There is a better way.
If medication supplementation is necessary, many patient’s insurance will now cover painlessly implantable sustained drug delivery options like durysta (bimatoprost pellet) or iDose (travoprost stent platform). Durysta was approved for 3 months of efficacy, but in studying my first 100 applications of the medication, I found that over 75% of patients achieved pressure control equivalent or better to their topical prostaglandin therapy through 6 months and a little over 50% kept control past 1 year. If Durysta has been successful, iDose is a natural next step as it can painlessly be implanted in minutes in our outpatient ambulatory surgical center achieving three or more years of pressure control.
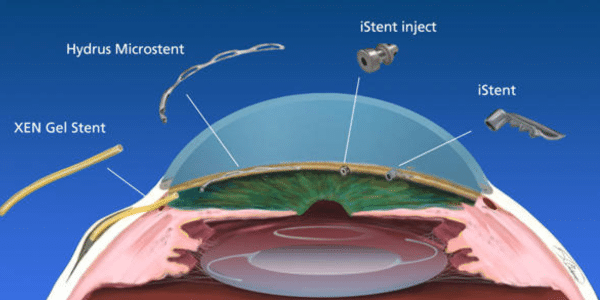
The last decade has also witnessed the proliferation of many safe minimally invasive glaucoma surgeries (MIGS), most commonly performed in conjunction with cataract surgery, and now, increasingly, also done stand alone. These procedures do not provide the very low intraocular pressures achieved by traditional filtration surgeries, but they show significant intraocular pressure lowering, decrease medication burden, and maintain an excellent safety profile. Each week many of our patients are receiving iStent infinite (3 stents), hydrus stent (3 clock hours stented), a four clock hour goniotomy, endoscopic cyclophotocoagulation (ECP), or controlled cyclodialysis cleft (alloflo). Having several options has helped me be able to tailor treatments to my patient’s specific circumstances. iStent is a preferred option in conjunction with cataract surgery with mild open angle glaucoma, goniotomy, ECP, and alloflo can be done in mild to advanced glaucomas, either standalone, or in conjunction with cataract surgery.
Of course, there are many patients I encounter who are uncontrolled, with more advanced glaucoma who necessitate filtration surgery; tube shunt or trabeculectomy. If this is needed, I have extensive experience in these procedures, and have modified my techniques over the years to optimize short and long term success, while minimizing complications. Using the antimetabolite, mitomycin C reduces fibroblast scarring around the filter, Ahmed valve minimizes risk for long term hypotony, as do Xen gel stent via poiseuille’s law, and Express mini shunt via its controlled 50 um internal opening. My closure technique reduces short term complications, like leakage, while maximizing long term bleb success.
It is my great pleasure to partner with my optometric and ophthalmic colleagues to help our glaucoma patients protect their sight.